Who are we?
Human Interventions are care consultants specialising in person centred interventions for people with mental disorders, including mental illness and dementia.
Human Interventions was created in 2018 by Walter and Shirley Brennan. They have over 80 years experience between them as mental health nurses, have published over 50 papers & articles, developed several risk assessment tools, delivering over 5000 days of training across the UK & Europe, and prepared thousands of expert witness statements.
Shirley is a former inspector of care homes and has extensive knowledge of dementia, confusion and the mis-use of restrictive physical interventions within care settings for older adults.
Human Interventions now have an excellent team of fully trained nurses and social care staff who all specialise in a wide range of ages delivering a high quality service for all requirements.


Our approach
Human Interventions specialises in health and care consultancy, offering tailored solutions across diverse settings such as hospitals, care homes, and residential facilities. Our independence enables us to assess each case objectively, providing recommendations solely in the individual’s best interest.
Our methodology enables us to work with various departments within the same organisation to meet the needs of all stakeholders whilst prioritising the individual’s best interests.
This approach enables commissioners to ensure accurate funding allocation while also ensuring that the care facility receives the necessary support and resources to cater to the person’s needs at the highest possible level.
Our work in 1-1 support has been pioneering within health and social care. We have developed action protocols for hospital discharge teams and care providers. We are working in partnership with ICBs & care providers to improve 1-1 support and enhanced observations through the use of evidential based and therapeutic interventions. We have published a number of articles on the use of 1-1 support and the use of restraint within care settings.
Historically 1-1 support within care settings has been viewed as a least restrictive intervention prescribed for people who present behaviours that challenge, including violence towards others or self, sexually inappropriate behaviour within communal settings, Pica and wandering into areas likely to result in conflict with other users.
However it is important to recognise that 1-1 support is a restrictive intervention and left unregulated it becomes just another method of restraint, often masquerading as care and when it results in people being isolated it can be described as ‘de facto seclusion’.
We look at 1-1 support as a potentially critical life enhancing measure. But when it is used as a knee jerk response to a sudden, short lived incident without consideration given to the impact on the person and their autonomy, our team will challenge the care providers and seek justification for its use.
We have carried out more than 400 1-1 reviews and assessments throughout the UK as we aim to ensure that valuable resources are allocated appropriately and also to promote recognition that 1-1 support is an intervention that should be meaningful, therapeutic appropriate for the person.
In 2019 we developed a method of data gathering for observers and carers. The Data Gathering Forms (DGFs) have been revised a number of times to make them more user friendly. Our DGF software, enables us to harvest data and present it in a cogent and easy read format supported by our innovative charts / graphs software technology.
There are two charts below. Figure one compares the disparity in recording incidents within a home. By identifying such inconsistencies it helps the care provider to improve data gathering and strive for accurate and better record keeping.
Figure 1
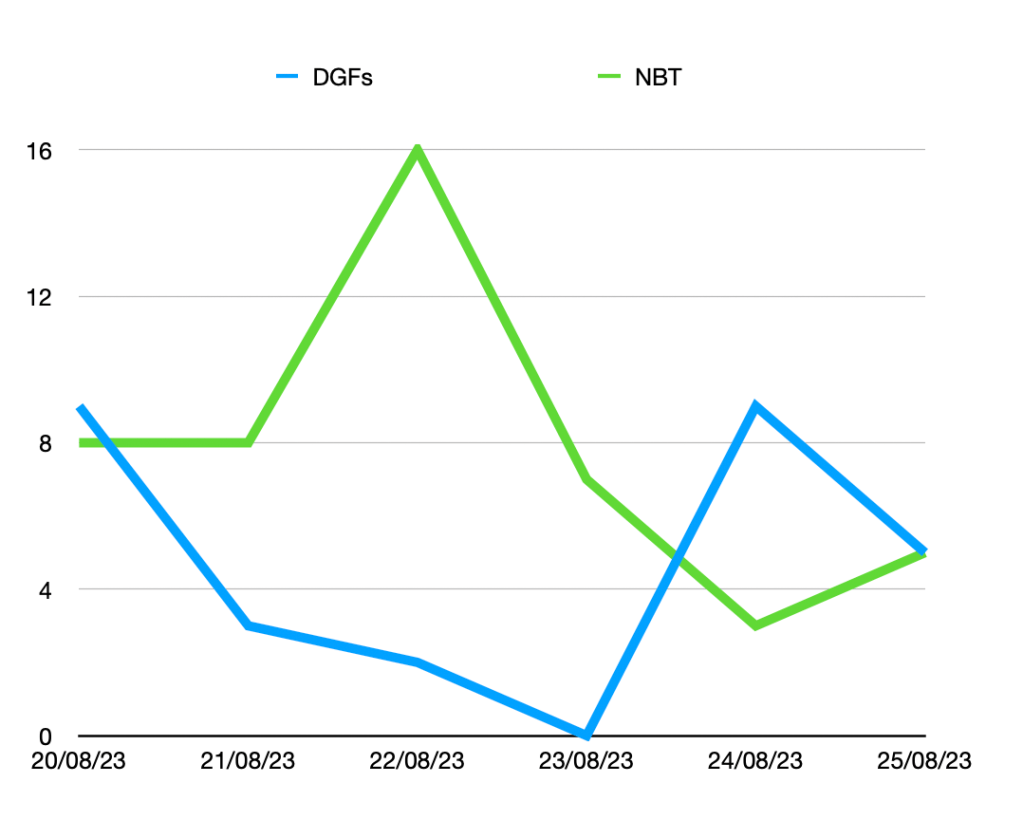
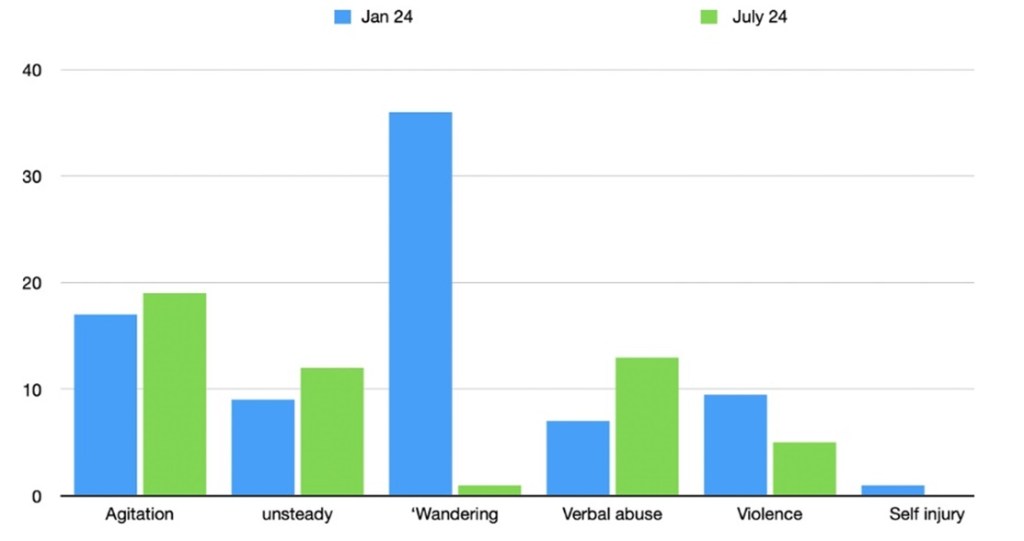
Figure 2
Figure 2 illustrate how a person’s behaviour will change over a period of time. This enables the care provider to help identify trends and themes for certain behaviours that may indicate a need for 1-1 support or a reduction of hours. It can be seen below that in this case whilst agitation, unsteadiness and verbal abuse have increased, violence towards others and wandering have decreased. The latter by a more than 90%.